
TL;DR:
- Longevity science focuses on understanding and modifying the biological mechanisms of aging to extend healthspan. It targets key hallmarks such as genomic instability, cellular senescence, and mTOR dysregulation using personalized, biomarker-driven interventions. Regular tracking of biological markers is essential for applying these advances effectively and safely.
Longevity science is defined as the interdisciplinary biological and medical study of aging mechanisms, aimed at extending healthspan rather than simply adding years to life. The field is grounded in the nine hallmarks of aging, a foundational framework covering genomic instability, cellular senescence, epigenetic changes, and deregulated nutrient sensing, among others. The National Institute on Aging recognizes these hallmarks as the core targets for diagnostics and interventions as of 2026. Where traditional medicine treats disease after it appears, longevity science targets the molecular processes that cause disease to appear in the first place. For anyone between 30 and 60 who wants to perform at a high level for decades, understanding this distinction is not academic. It is operational.
What is longevity science and how does it work biologically?
Longevity science operates at the cellular and molecular level. Its central claim is that aging is not a passive process but a set of measurable, partially modifiable biological events. The nine hallmarks of aging serve as the field's working map, identifying the specific mechanisms that drive functional decline over time.

The hallmarks that matter most
Several hallmarks carry particular weight for men in high-output roles:
- Genomic instability: DNA accumulates damage over time from oxidative stress, radiation, and replication errors. Cells with damaged DNA either malfunction or trigger inflammatory responses.
- Cellular senescence: Damaged cells stop dividing but refuse to die. They release inflammatory signals, a process researchers call the senescence-associated secretory phenotype (SASP), which degrades surrounding tissue and accelerates systemic aging.
- Epigenetic changes: Gene expression patterns shift with age, silencing protective genes and activating harmful ones. Epigenetic clocks, such as the Horvath clock, can now measure biological age with meaningful accuracy.
- Deregulated nutrient sensing: Pathways like mTOR and IGF-1 govern how cells respond to food and energy. Chronic overactivation of mTOR, common in high-calorie Western diets, accelerates cellular aging.
- Mitochondrial dysfunction: Mitochondria lose efficiency with age, producing less energy and more cellular waste. This shows up as fatigue, cognitive fog, and reduced physical capacity.
Genetics also shape how these hallmarks progress. Genes like PSRC1 and CASP8 are linked to longevity through lipid metabolism and immune regulation pathways. That means your biological trajectory is partly inherited, though it is far from fixed.
Pro Tip: If you want a concrete starting point, ask your physician for an epigenetic age test alongside standard bloodwork. The gap between your chronological age and your biological age tells you more than any single biomarker.
How does longevity science differ from traditional medicine?
Traditional medicine is reactive. It waits for a diagnosis, then treats the condition. Longevity science is proactive. It monitors the rate of biological aging before disease appears and intervenes at the molecular level to slow that rate.
The practical difference shows up in the tools used. Standard annual check-ups measure cholesterol, blood pressure, and blood glucose. Longevity medicine adds epigenetic clocks and multi-omics profiling, which track biological aging across genomic, proteomic, and metabolomic dimensions simultaneously. This creates a high-resolution picture of where your body is aging fastest.
The goal is also different. Longevity science does not aim for indefinite lifespan. It aims to compress morbidity, meaning it works to reduce the period of illness and functional decline at the end of life, so that vitality extends as close to the end as possible. The distinction between healthspan and lifespan is central here. Lifespan is how long you live. Healthspan is how long you live well.
Four principles separate longevity medicine from wellness trends:
- Mechanistic targets: Interventions must address a specific hallmark of aging, not a vague concept like "detox" or "balance."
- Biomarker validation: Effects must be measurable through objective biological markers, not self-reported wellbeing alone.
- Longitudinal monitoring: A single data point means nothing. Tracking biological age over time reveals whether an intervention is working.
- Individual calibration: What works for one person may not work for another due to genetic and metabolic differences. Personalization is not optional.
Skepticism toward unproven supplements and generalized wellness claims is built into the discipline. Longevity medicine moves beyond reactive disease treatment toward managing the molecular rate of aging itself.
What does the evidence say about longevity interventions?
The National Institute on Aging's Interventions Testing Program (ITP) has tested over 50 compounds in animal models, with roughly 25% showing lifespan extension effects. That is a meaningful signal, but it also means 75% did not perform. The rigor of the ITP is precisely what separates longevity research from supplement marketing.
Rapamycin stands out as the most studied compound in this space. It inhibits mTORC1, the nutrient-sensing pathway most associated with accelerated aging, and shows significant pro-longevity effects in both sexes, even when administered late in life. That finding is notable because most interventions lose efficacy when started after middle age.
Dietary restriction is another well-documented pathway. Caloric restriction modulates mTORC1 and NAD+ metabolism, two of the most studied molecular targets in aging research. The evidence from animal models is strong. The human application is more complex.
| Intervention | Mechanism | Evidence Level | Key Trade-off |
|---|---|---|---|
| Rapamycin | mTOR inhibition | Strong (animal); emerging (human) | Immune suppression risk |
| Caloric restriction | mTOR, NAD+ modulation | Strong (animal); mixed (human) | Infection susceptibility |
| NAD+ precursors | Mitochondrial support | Moderate | Long-term human data limited |
| Epigenetic reprogramming | Hallmark reversal | Early-stage | Translational complexity |
Animal model findings do not translate directly to humans. Sex- and age-dependent effects on longevity-related genes mean that a compound effective in male mice at age 12 months may behave differently in a 55-year-old man. The field is aware of this gap and actively working to close it.
Pro Tip: Dietary restriction carries real immune risks if applied without monitoring. Before adjusting caloric intake for longevity purposes, establish baseline metabolic and immune markers so you can track the biological effect, not just the scale.
How can you apply longevity science to your own healthspan?
The gap between laboratory findings and personal practice is where most people get lost. Applying longevity science to your own biology requires moving beyond generic health advice and into personalized, data-driven territory.
Start with diagnostics that go beyond the standard annual panel:
- Epigenetic age testing: Measures biological age against chronological age using DNA methylation patterns. A meaningful gap in either direction tells you whether your current lifestyle is accelerating or slowing your aging rate.
- Metabolomic profiling: Identifies how your body processes nutrients, hormones, and inflammatory signals. This reveals individual variation that generic nutrition advice cannot account for.
- Inflammatory marker tracking: Chronic low-grade inflammation, sometimes called inflammaging, is a driver of multiple hallmarks. CRP, IL-6, and TNF-alpha are measurable and modifiable.
- Telomere length assessment: Provides a secondary indicator of cellular aging, most useful when tracked longitudinally rather than as a single reading.
Lifestyle factors aligned with longevity science are not exotic. Longevity lifestyle practices that consistently show up in the research include resistance training, time-restricted eating, sleep quality optimization, and stress regulation through measurable HRV tracking. These are not wellness trends. They are interventions with known molecular mechanisms.
Genetic individuality matters here. Personalized longevity strategies must account for your specific metabolic and genetic profile to avoid unintended trade-offs. A high-fat diet that improves metabolic markers in one person may worsen lipid profiles in another due to APOE genotype variation. The same principle applies to fasting protocols, supplementation, and exercise intensity.
For professionals focused on healthspan, the practical priority is consistent monitoring. One data point is noise. A trend line over 12–24 months is signal. Build the habit of tracking biological markers the same way you track business metrics.
Key Takeaways
Longevity science is the only medical discipline that targets aging itself rather than its downstream diseases, making it the most relevant framework for anyone who wants to remain functional and sharp well into later decades.
| Point | Details |
|---|---|
| Healthspan over lifespan | The goal is compressing morbidity, not simply adding years to life. |
| Nine hallmarks as the map | Genomic instability, senescence, and mTOR dysregulation are the primary targets for intervention. |
| Biomarker tracking is non-negotiable | Epigenetic clocks and multi-omics profiling replace guesswork with measurable biological data. |
| Personalization determines outcomes | Genetic and metabolic individuality means no single protocol works for everyone. |
| Evidence has limits | Animal model findings require careful translation; interventions like rapamycin carry real trade-offs. |
Where I think most people get this wrong
Most men I talk to in high-performance roles approach longevity the way they approach a business problem: find the best solution, implement it, move on. That instinct fails here, and I say that from direct experience with biomarker tracking over several years.
The biology does not reward one-time optimization. It rewards consistency and recalibration. I have seen men with excellent baseline markers deteriorate over 18 months because they treated an intervention as a fixed protocol rather than a living variable. Rapamycin is a good example. The biological trade-offs around immune function are real, and they are not visible without monitoring. The men who benefit most from longevity science are the ones who treat their biology as a data system, not a machine to be tuned once.
The other mistake is conflating longevity science with wellness culture. They are not the same discipline. Wellness sells feeling better. Longevity science measures whether you are actually aging more slowly. The shift from trend-based wellness to targeting the hallmarks of aging through biological markers is the defining move. Make that shift, and the rest of the field starts to make sense.
My honest position: cautious optimism grounded in data. The science is real, the progress is meaningful, and the tools available in 2026 are genuinely better than they were a decade ago. But no compound, protocol, or device replaces longitudinal self-knowledge. That is the edge that actually compounds.
— Joakim
Viridos and the discipline of tracking what matters
Longevity science without consistent tracking is theory. The men who make measurable progress are the ones who build a disciplined system for monitoring their biological markers, performance outputs, and recovery patterns over time.
Viridos developed the Performance Journal for exactly this purpose. It is a premium tool built for founders, executives, and high-agency professionals who want to apply longevity science principles to their daily performance. The journal structures the kind of longitudinal self-monitoring that separates serious practitioners from casual wellness consumers. If you are ready to move from reading about modern longevity tools to using them with discipline, the Performance Journal is the place to start.
FAQ
What is longevity science in simple terms?
Longevity science is the biological and medical study of how and why we age, with the goal of extending the healthy years of life. It targets specific cellular and molecular mechanisms rather than treating individual diseases after they appear.
What is the difference between healthspan and lifespan?
Lifespan is the total number of years lived. Healthspan is the number of years lived in good functional health, free from significant disease or decline. Longevity science prioritizes healthspan by working to compress the period of illness at the end of life.
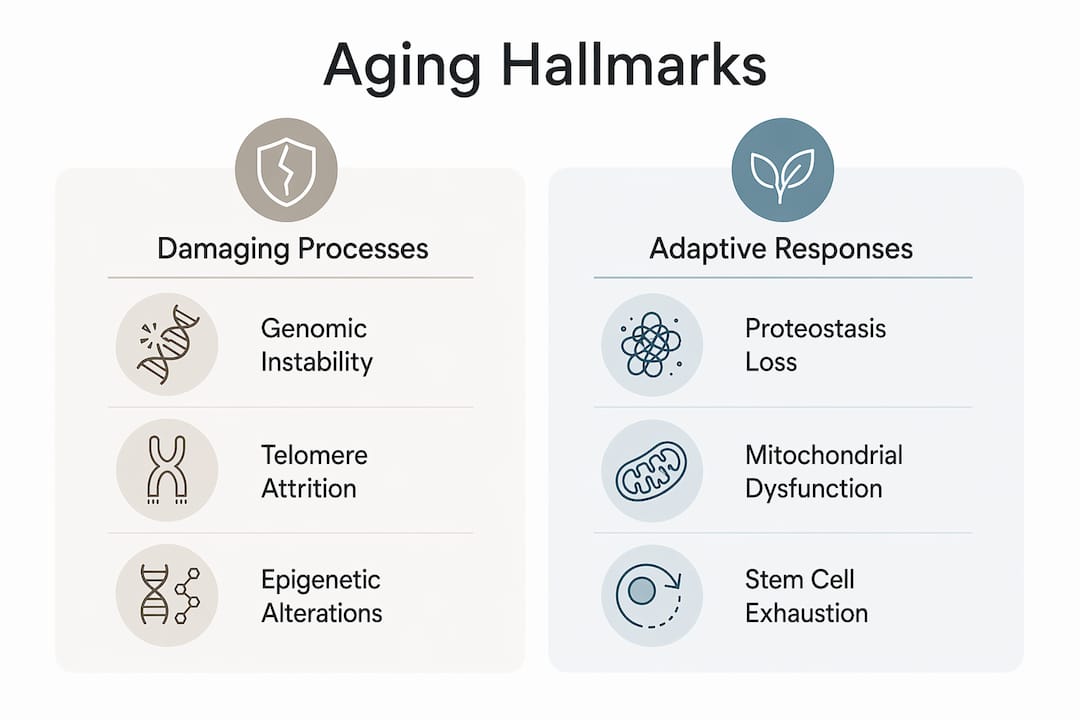
What are the nine hallmarks of aging?
The nine hallmarks of aging are genomic instability, telomere attrition, epigenetic changes, loss of proteostasis, deregulated nutrient sensing, mitochondrial dysfunction, cellular senescence, stem cell exhaustion, and altered intercellular communication. They represent the core biological mechanisms driving age-related decline.
Does genetics determine how long you live?
Genetics influence longevity through pathways in lipid metabolism, immune regulation, and IGF-1 signaling, but they do not determine outcomes alone. Lifestyle, environment, and targeted interventions can modify how these genetic factors express over time.
Is rapamycin safe for longevity purposes?
Rapamycin shows strong pro-longevity effects in animal models and emerging evidence in humans, but it carries immune suppression risks that require medical monitoring. It is not a self-administered supplement and should only be considered under physician supervision with regular biomarker tracking.